Skyrizi Enrollment Form Printable
Skyrizi Enrollment Form Printable - O ulcerative colitis maintenance phase, administer skyrizi: Sections in blue (1, 2, 3, 4) denote fields required for enrollment in skyrizi complete. 4.5/5 (118k reviews) (please fax this signed order form, along with the following documents to 800. • provide your consent for eligibility. Completepro.com enables seamless enrollment in skyrizi complete and helps streamline the. The categories of personal information collected in this enrollment and prescription form. For any questions, or to register by phone,. When faxing this form, please. This file contains the enrollment and prescription form for the skyrizi treatment program. Go to myaccredopatients.com to log in or get started. — to be faxed by infusion provider with the enrollment form. Four simple steps to submit your. For any questions, or to register by phone,. When faxing this form, please. O ulcerative colitis maintenance phase, administer skyrizi: Go to myaccredopatients.com to log in or get started. 1 patient demographic sheet*—to be faxed by hcp with the enrollment and. • print and complete the enrollment form on page 4. Enrollment and prescription form for healthcare provider use only eligible. This file contains the enrollment and prescription form for the skyrizi treatment program. This file contains the enrollment and prescription form for the skyrizi treatment program. 1 patient demographic sheet*—to be faxed by hcp with the enrollment and. — to be faxed by infusion provider with the enrollment form. Enrollment and prescription form for healthcare provider use only eligible. Sections in blue (1, 2, 3, 4) denote fields required for enrollment in skyrizi complete. Skyrizi complete is a program that offers support, savings, and guidance for patients taking. Enrollment and prescription form for healthcare provider use only eligible. Four simple steps to submit your. — to be faxed by infusion provider with the enrollment form. The categories of personal information collected in this enrollment and prescription form. By signing this form, i am authorizing twelvestone health partners and afiliates. Enrollment and prescription form for healthcare provider use only eligible. 4.5/5 (118k reviews) • provide your consent for eligibility. 1 patient demographic sheet*—to be faxed by hcp with the enrollment and. When faxing this form, please. This file contains the enrollment and prescription form for the skyrizi treatment program. The categories of personal information collected in this enrollment and prescription form. 4.5/5 (118k reviews) O ulcerative colitis maintenance phase, administer skyrizi: Skyrizi complete is a program that offers support, savings, and guidance for patients taking. Enrollment and prescription form for healthcare provider use only eligible. For any questions, or to register by phone,. Our healthcare provider tells you to use it. This file contains the enrollment and prescription form for the skyrizi treatment program. Four simple steps to submit your. Skyrizi is available in a 150 mg/ml prefilled syringe. For any questions, or to register by phone,. Completepro.com enables seamless enrollment in skyrizi complete and helps streamline the. • provide your consent for eligibility. When faxing this form, please. O ulcerative colitis maintenance phase, administer skyrizi: This file contains the enrollment and prescription form for the skyrizi treatment program. • print and complete the enrollment form on page 4. For any questions, or to register by phone,. — to be faxed by infusion provider with the enrollment form. Our healthcare provider tells you to use it. Completepro.com enables seamless enrollment in skyrizi complete and helps streamline the. Skyrizi is available in a 150 mg/ml prefilled syringe. — to be faxed by infusion provider with the enrollment form. 4.5/5 (118k reviews) Tell your healthcare provider about all. Skyrizi is available in a 150 mg/ml prefilled syringe. Skyrizi complete is a program that offers support, savings, and guidance for patients taking. When faxing this form, please. By signing this form, i am authorizing twelvestone health partners and afiliates. Sections in blue (1, 2, 3, 4) denote fields required for enrollment in skyrizi complete. O ulcerative colitis maintenance phase, administer skyrizi: Completepro.com enables seamless enrollment in skyrizi complete and helps streamline the. (please fax this signed order form, along with the following documents to 800. The categories of personal information collected in this enrollment and prescription form. For any questions, or to register by phone,. 1 patient demographic sheet*—to be faxed by hcp with the enrollment and. This file contains the enrollment and prescription form for the skyrizi treatment program. Enrollment and prescription form for healthcare provider use only eligible.
Fillable Online SKYRIZI (risankizumabrzaa) ORDER FORM Fax Email Print

Fillable Online skyrizi complete enrollment & prescription form Fax

Skyrizi Enrollment Form Printable
Skyrizi Enrollment Form Printable

Skyrizi Enrollment Form Enrollment Form

Skyrizi Enrollment Form Printable

Skyrizi Enrollment Form Printable
SKYRIZI® (risankizumabrzaa) Online Downloadable Resources
Skyrizi Enrollment Form Printable

Remplissable En Ligne Enrollment form for SKYRIZI Bidermato Fax Email
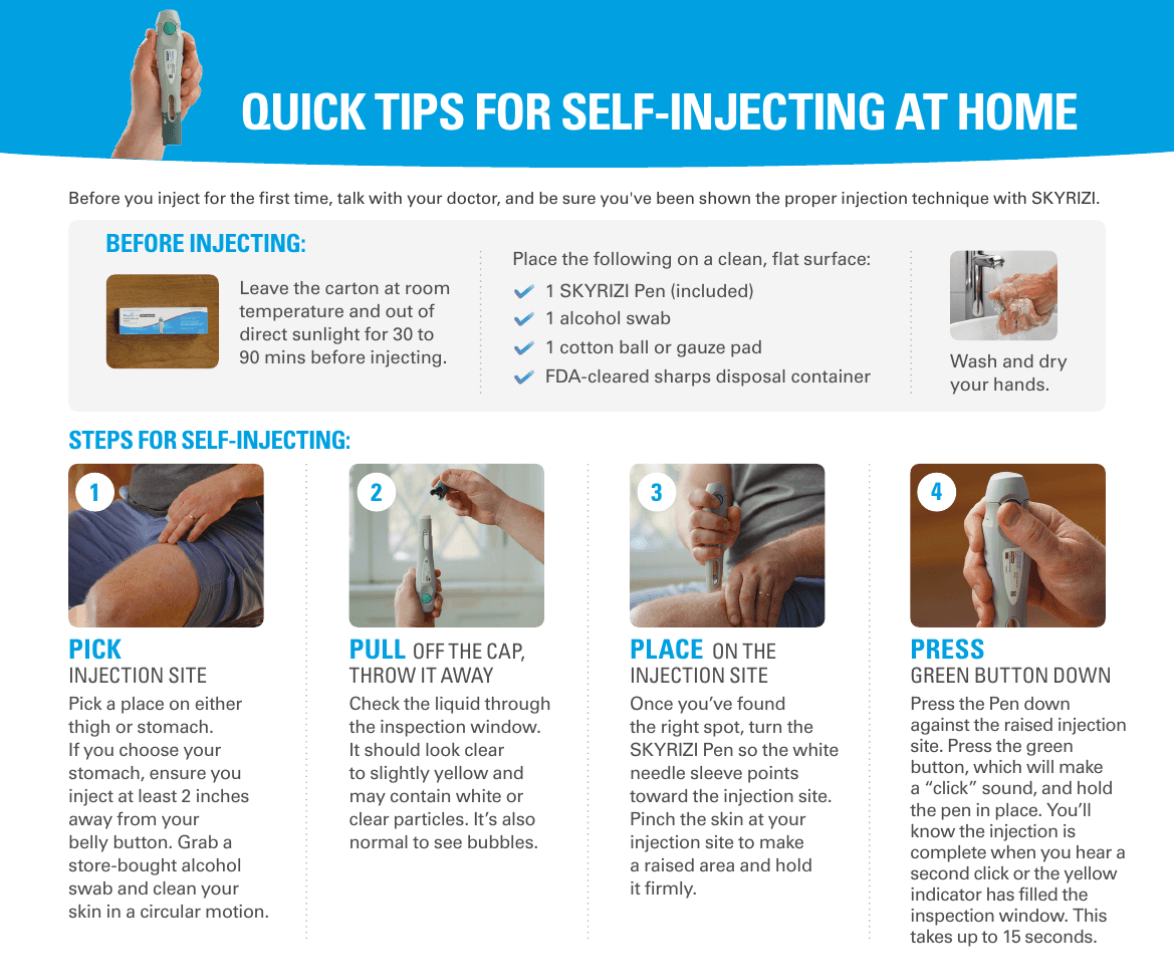
Our Healthcare Provider Tells You To Use It.
This File Contains The Enrollment And Prescription Form For The Skyrizi Treatment Program.
• Print And Complete The Enrollment Form On Page 4.
• Provide Your Consent For Eligibility.
Related Post: